The Novavax COVID-19 vaccine is a protein subunit COVID-19 vaccine that is authorized for use in the United States under Emergency Use Authorization. Learn more about Novavax COVID-19 vaccine, including who can get it, doses, and ingredients.
How Protein Subunit COVID-19 Vaccines Work
Protein subunit vaccines contain pieces (proteins) of the virus that causes COVID-19. These virus pieces are the spike protein. The vaccine also contains another ingredient called an adjuvant that helps the immune system respond to that spike protein in the future. Once the immune system knows how to respond to the spike protein, the immune system will be able to respond quickly to the actual virus spike protein and protect you against COVID-19.
First, protein subunit COVID-19 vaccines are given in the upper arm muscle. After vaccination, nearby cells pick up these proteins.
Next, our immune system recognizes that these proteins do not belong there. Another ingredient in the vaccine, the adjuvant, helps our immune system to produce antibodies and activate other immune cells to fight off what it thinks is an infection. This is what your body might do if you got sick with COVID-19.
At the end of the process, our bodies have learned how to help protect against future infection with the virus that causes COVID-19. The benefit is that people get this protection from a vaccine, without ever having to risk the potentially serious consequences of getting sick with COVID-19. Many side effects from getting the vaccine are normal signs the body is building protection.
Facts About Protein Subunit COVID-19 Vaccines
Protein subunit COVID-19 vaccines cannot cause COVID-19 or other illnesses.
Protein subunit COVID-19 vaccines do not use any live virus.
Protein subunit COVID-19 vaccines cannot cause infection with the virus that causes COVID-19 or other viruses.
They do not affect or interact with our DNA.
The protein pieces do not enter the nucleus of the cell where our DNA (genetic material) is located, so they cannot change or influence our genes.
Protein Subunit COVID-19 Vaccines Have Been Rigorously Evaluated for Safety
Protein subunit COVID-19 vaccines have been held to the same rigorous safety and effectiveness standards as all other types of vaccines in the United States. The only COVID-19 vaccines the Food and Drug Administration (FDA) makes available for use in the United States (by approval or emergency use authorization) are those that meet these standards.
Protein Subunit Vaccines Have Been Used for Years
More than 30 years ago, a hepatitis B vaccine became the first protein subunit vaccine to be approved for use in people in the United States. Another example of other protein subunit vaccines used in the United States today include acellular pertussis (whooping cough) vaccines.
To learn more, please visit https://www.cdc.gov/coronavirus/2019-ncov/vaccines/different-vaccines/proteinsubunit.html
COVID-19 vaccines help protect against severe illness, hospitalization and death. COVID-19 vaccines also help protect against infection. People who are vaccinated may still get COVID-19. When people who have been vaccinated get COVID-19, they are much less likely to experience severe symptoms than people who are unvaccinated.
When someone who is vaccinated with either a primary series or a primary series plus a booster dose gets infected with the virus that causes COVID-19, it is referred to as a “vaccine breakthrough infection.”
When people who are vaccinated get COVID-19 get a breakthrough infection, they are much less likely to experience severe symptoms than people who are unvaccinated.
People who get vaccine breakthrough infections can spread COVID-19 to other people. When a community reports more COVID-19 infections, that means more virus is circulating. When more virus is circulating, more breakthrough infections will occur even when vaccination rates are high. Even if you are vaccinated, if you live in a county with a high COVID-19 Community Level, you and others in your community, whether vaccinated or not, should take more steps to protect yourself and others, like wearing a mask in indoor public places.
CDC monitors reported vaccine breakthrough infections to better understand patterns of COVID-19 among people who are vaccinated and unvaccinated. The latest rates of COVID-19 cases and deaths by vaccination status are available on the CDC COVID Data Tracker.
To learn more, please visit https://www.cdc.gov/coronavirus/2019-ncov/vaccines/effectiveness/why-measure-effectiveness/breakthrough-cases.html
Residential communities for older adults may combine nursing, assisted living, and independent living lifestyles. Each community may face different risks and decide to put in place less restrictive or more restrictive protocols.
Learn more about the risks among people who live in nursing homes or long-term care facilities and about CDC’s guidance for preventing the spread COVID-19 infection in nursing homes.
There is no way to ensure you have zero risk of getting the virus that causes COVID-19. So, it is important to understand the risks and know how to reduce your risk as much as possible if or when you do resume some activities, run errands, and attend events and gatherings.
While it is generally safest to implement universal use of source control for everyone in a healthcare setting, the following allowances could be considered for individuals who are up to date with all recommended COVID-19 vaccine doses (who do not otherwise meet the criteria described above) in healthcare facilities located in counties with low to moderate community transmission. These individuals might choose to continue using source control if they or someone in their household is immunocompromised or at increased risk for severe disease, or if someone in their household is not up to date with all recommended COVID-19 vaccine doses.
HCP who are up to date with all recommended COVID-19 vaccine doses:
Could choose not to wear source control or physically distance when they are in well-defined areas that are restricted from patient access (e.g., staff meeting rooms, kitchen).
They should wear source control when they are in areas of the healthcare facility where they could encounter patients (e.g., hospital cafeteria, common halls/corridors).
Patient Visitation:
Indoor visitation (in single-person rooms; in multi-person rooms, when roommates are not present; or in designated visitation areas when others are not present): The safest practice is for patients and visitors to wear source control and physically distance, particularly if either of them are at risk for severe disease or are unvaccinated.
If the patient and all their visitor(s) are up to date with all recommended COVID-19 vaccine doses, they can choose not to wear source control and to have physical contact.
Visitors should wear source control when around other residents or HCP, regardless of vaccination status.
Outdoor Visitation: Patients and their visitors should follow the source control and physical distancing recommendations for outdoor settings described on the page addressing Your Guide to Masks.
Residents who are up to date with all recommended COVID-19 vaccine doses in Nursing Homes in Areas of Low to Moderate Transmission:
Nursing homes are healthcare settings, but they also serve as a home for long-stay residents and quality of life should be balanced with risks for transmission. In light of this, consideration could be given to allowing residents who are up to date with all recommended COVID-19 vaccine doses to not use source control when in communal areas of the facility; however, residents at increased risk for severe disease should still consider continuing to practice physical distancing and use of source control
The Pfizer-BioNTech and Moderna COVID-19 vaccines are messenger RNA vaccines, also called mRNA vaccines. Learn more about Pfizer-BioNTech and Moderna COVID-19 vaccines, including who can get them, doses, and ingredients.
How mRNA COVID-19 Vaccines Work
To trigger an immune response, many vaccines put a weakened or inactivated germ into our bodies. Not mRNA vaccines. Instead, mRNA vaccines use mRNA created in a laboratory to teach our cells how to make a protein—or even just a piece of a protein—that triggers an immune response inside our bodies. That immune response, which produces antibodies, is what helps protect us from getting sick from that germ in the future.
First, mRNA COVID-19 vaccines are given in the upper arm muscle. After vaccination, the mRNA will enter the muscle cells. Once inside, they use the cells’ machinery to produce a harmless piece of what is called the spike protein. The spike protein is found on the surface of the virus that causes COVID-19. After the protein piece is made, our cells break down the mRNA and remove it.
Next, our cells display the spike protein piece on their surface. Our immune system recognizes that the protein does not belong there. This triggers our immune system to produce antibodies and activate other immune cells to fight off what it thinks is an infection. This is what your body might do if you got sick with COVID-19.
At the end of the process, our bodies have learned how to help protect against future infection with the virus that causes COVID-19. The benefit is that people get this protection from a vaccine, without ever having to risk the potentially serious consequences of getting sick with COVID-19. Any side effects from getting the vaccine are normal signs the body is building protection.
mRNA COVID-19 Vaccines Have Been Rigorously Evaluated for Safety
mRNA COVID-19 vaccines have been held to the same rigorous safety and effectiveness standards as all other types of vaccines in the United States. The only COVID-19 vaccines the Food and Drug Administration (FDA) makes available for use in the United States (by approval or emergency use authorization) are those that meet these standards.
mRNA Vaccines Are Newly Available to the Public, but Have Been Studied for Decades
Researchers have been studying and working with mRNA vaccines for decades. Interest has grown in these vaccines because they can be developed in a laboratory using readily available materials. This means vaccines can be developed and produced in large quantities faster than with other methods for making vaccines.
mRNA vaccines have been studied before for flu, Zika, rabies, and cytomegalovirus (CMV). As soon as the necessary information about the virus that causes COVID-19 was available, scientists began designing the mRNA instructions for cells to build the unique spike protein into an mRNA vaccine.
Future mRNA vaccine technology may allow for one vaccine to provide protection against multiple diseases, thus decreasing the number of shots needed for protection against common vaccine-preventable diseases.
Beyond vaccines, cancer research has used mRNA to trigger the immune system to target specific cancer cells.
COVID-19 vaccines are available for everyone ages 5 years and older at no cost.
Vaccines were paid for with taxpayer dollars and will be given free of charge to all people living in the United States, regardless of insurance or immigration status.
COVID-19 vaccination is an important tool to help stop the pandemic.
If anyone asks you to pay for access to a COVID-19 vaccine, you can bet it’s a scam. Don’t share your personal or financial information if someone calls, texts, or emails you promising access to a vaccine for an extra fee.
COVID-19 vaccination providers cannot:
Charge you for a vaccine
Charge you directly for any administration fees, copays, or coinsurance
Deny vaccination to anyone who does not have health insurance coverage, is underinsured, or is out of network
Charge an office visit or other fee to the recipient if the only service provided is a COVID-19 vaccination
Require additional services in order for a person to receive a COVID-19 vaccine; however, additional healthcare services can be provided at the same time and billed as appropriate
COVID-19 vaccination providers can:
Seek appropriate reimbursement from the recipient’s plan or program (e.g., private health insurance, Medicare, Medicaid) for a vaccine administration fee
However, providers cannot charge the vaccine recipient the balance of the bill.
Anyone in the United States Can Get Vaccinated
The federal government is providing vaccines free of charge to everyone 5 years and older living in the United States, regardless of their immigration or health insurance status.
CDC does not require U.S. citizenship for individuals to receive a COVID-19 vaccine. Jurisdictions (state, tribal, local, and territorial) cannot add U.S. citizenship requirements or require U.S. citizenship verification as a requirement for vaccination.
Pursue telehealth as an alternative to face-to-face healthcare services, commonly used pre-pandemic, to:
Reduce unnecessary exposure to COVID-19,
Help mitigate the spread of the virus, and
Reduce surges in hospitals and clinics.
This guidance document is developed to encourage healthcare providers to explore ways of meeting the essential healthcare needs of the community using innovative telehealth modalities and technologies; and expand the use of telehealth in the care of patients, and telemedicine in the care of COVID-19 and other non-COVID-19 patients.
WHAT IS TELEHEALTH?
Telehealth is remote patient care and monitoring. It allows direct transmission of a patient’s clinical measurements from a distance to their healthcare provider and may or may not be in real time. The telehealth session may also be facilitated by a Healthcare Professional (to other healthcare professionals), Village Health Volunteer -VHV, a Community Health Worker -CHW visiting the patient, or by the patient him/her-self, a parent or a legal guardian. Telehealth can be any combination of healthcare services including telemedicine. Some healthcare specialties default to “referring to all of such services” as telehealth. “TeleCOVID-19” care is Telemedicine.
Examples of Telehealth Care include:
Screening for COVID-19, testing recommendations, and guidance on isolation or quarantine
General health care (i.e. wellness visits, blood pressure control, advice about certain non-emergency illnesses, like common rashes)
Non-emergency follow-up clinics
Prescriptions for medication
Nutrition counseling
Mental health counseling
Physical therapy exercise
Teleradiology
Tele-intensive care (in infectious disease hospitalizations)
Telemedicine
Telehealth decreases contact with healthcare facilities, other patients, and healthcare staff in order to reduce the risk of COVID-19 spread in the community.
Generally, Telehealth Modalities include:
Synchronous: Real-time telephone or live audio-video interaction, typically with a patient, using a smartphone, tablet, or computer.
For example: In some cases, peripheral medical equipment (e.g., digital stethoscopes, otoscopes, ultrasounds) can be used by another health care provider (e.g., nurse, medical assistant) physically with the patient, while the consulting medical provider conducts a remote evaluation.
Asynchronous:The provider and patient communication does not happen in real time.
For example, “store and forward” technology allows messages, images, or data to be collected at one point in time and interpreted or responded to later. Patient portals can facilitate this type of communication between provider and patient through secure messaging. Other examples of telehealth modalities developed/used by American College of Obstetricians and Gynecologistsexternal icon include:
Live, two-way (or real-time) synchronous audio and video allows specialists, local physicians, and patients to see and hear each other in real-time to discuss conditions e.g. via phone or computer (also defined above).
Store-and-forward, also referred to as “asynchronous telemedicine,” sends medical imaging such as X-rays, photos, ultrasound recordings, or other static and video medical imaging to remote specialists for analysis and future consultation (also defined above).
Remote patient monitoring collects personal health and medical data from a patient in one location and electronically transmits the data to a physician in a different location for use in care and related support.
mHealth is a general term for self-managed patient care using mobile phones or other wireless technology and does not necessarily involve monitoring by a physician. It is most commonly used to deliver or reinforce patient education about preventive care and provide medication reminders, appointment reminders, and other essential self-care steps that patients should undertake to maintain their optimal obstetric health.
WHAT IS TELEMEDICINE?
Telemedicine is the use of electronic information and telecommunication technology to get needed health care while practicing physical distancing. This encourages meaningful use of patient health measures to help guide the engagement of patient in care.
Remote diagnosing and teleconsulting* system. Data (including signals and images) are locally (patient-side) acquired and stored, and then forwarded to the main hospital, where physicians can analyze those data. The remote (physician-side) hospital will then send back the diagnosis.
Remote diagnosis performed with patient assisted by nurses. If no physician is in the neighborhood: such a situation typically occurs in rural locations of developing countries, and in some cases a preliminary diagnosis is locally performed by the aid of a decision support system (DSS).
Remote monitoring system. The patient is monitored in the remote location, his/her signals are continuously acquired, forwarded to the main hospital, and possibly, locally analyzed by a DSS. Alarms are remotely detected and transmitted back to the patient-side. The monitoring system can be managed and locally controlled by a physician or by a nurse.
Remote intervention system. The patient enters the operating room, the intervention is performed through a local (patient-side) robot that is remotely controlled by a physician in the main hospital. The remote intervention requires that some local assistance is performed by a physician or by a nurse.
Remote education (e-learning) system. Students or caregivers (mostly physicians, nurses, and technicians) attend classes taught from remote academic institutions, and possibly by a bi-directional communication interact with the teacher by making up questions. Remote education can be locally assisted by a local tutor, during and/or after the classes.
*Note: Teleconsulting, i.e., expert second opinion, is performed among physicians, where a non-specialist physician requires a remote consultation with one or more specialist physicians: typically, such a situation occurs in emergency centers of rural locations or in minor hospitals of developed countries, or in any location of developing countries.
POTENTIAL LIMITATIONS OF TELEHEALTH
Adaptations to telehealth may need to be considered in certain situations where in-person visits are more appropriate such as:
Due to urgency, a person’s underlying health conditions, or the fact that a physical exam or laboratory testing is needed for medical decision making.
If sensitive topics need to be addressed, especially if there is patient discomfort or concern for privacy.
Limited access to technological devices (e.g., phones, tablets, computers) or connectivity. This may be especially true for those living in rural settings.
When healthcare workers or patients may be less comfortable with using the technology, and may prefer an in-person visit.
When virtual visits are not readily accepted in lieu of in-person visits by healthcare workers or patients.
The federal government is committed to ensuring that residents and staff in long-term care (LTC) settings, such as nursing homes, assisted living, residential care communities, group homes and senior housing, have access to COVID-19 vaccines to receive primary series and booster shots. For additional examples of LTC settings, see COVID-19 Vaccine Access in Long-Term Care Settingsexternal icon.
The goal is to continue to protect those who are disproportionately affected by COVID-19—especially residents of LTC settings. All LTC settings that request assistance accessing COVID-19 vaccines for their residents and staff will receive the support they need.
Many LTC providers have already identified strategies and partnerships to obtain and administer COVID-19 vaccines for residents and staff. These include:
Coordinating with state and local health departments
Long-term care providers are encouraged to consider the option that works best for their residents and staff when coordinating access to COVID-19 vaccines, either in the local community or on-site. Additional details on these options are available on the pages linked below.https://www.cdc.gov/vaccines/covid-19/long-term-care/pharmacy-partnerships/administrators-managers.htmlhttps://www.cdc.gov/vaccines/covid-19/long-term-care/pharmacy-partnerships/jurisdictions.html
Additional Information COVID-19 Vaccination Recommendations
COVID-19 vaccination is recommended for all people ages 5 years and older in the United States for the prevention of COVID-19. COVID-19 vaccines currently approved or authorized by FDA are highly effective in preventing serious outcomes of COVID-19, including severe disease, hospitalization, and death. Efforts to maximize the proportion of people in the United States who are fully vaccinated against COVID-19 remain critical to ending the COVID-19 pandemic. At present, people with moderately to severely compromised immune systems should receive an additional dose of mRNA COVID-19 vaccine after the initial 2 doses.
In addition, COVID-19 vaccines may now be administered along with other vaccines. This includes simultaneous administration of the COVID-19 vaccine and other vaccines such as the flu vaccine on the same day, as well as coadministration within 14 days. For more information, see Interim Clinical Considerations for Use of COVID-19 Vaccines.
Some people who have been infected with the virus that causes COVID-19 can experience long-term effects from their infection, known as post-COVID conditions (PCC) or long COVID.
People call post-COVID conditions by many names, including: long COVID, long-haul COVID, post-acute COVID-19, post-acute sequelae of SARS CoV-2 infection (PASC), long-term effects of COVID, and chronic COVID.
WHAT YOU NEED TO KNOW
Post-COVID conditions can include a wide range of ongoing health problems; these conditions can last weeks, months, or years.
Post-COVID conditions are found more often in people who had severe COVID-19 illness, but anyone who has been infected with the virus that causes COVID-19 can experience post-COVID conditions, even people who had mild illness or no symptoms from COVID-19.
People who are not vaccinated against COVID-19 and become infected may also be at higher risk of developing post-COVID conditions compared to people who were vaccinated and had breakthrough infections.
There is no single test for post-COVID conditions. While most people with post-COVID conditions have evidence of infection or COVID-19 illness, in some cases, a person with post-COVID conditions may not have tested positive for the virus or known they were infected.
CDC and partners are working to understand more about who experiences post-COVID conditions and why, including whether groups disproportionately impacted by COVID-19 are at higher risk.
ABOUT LONG COVID OR POST-COVID CONDITIONS
Post-COVID conditions are a wide range of new, returning, or ongoing health problems that people experience after first being infected with the virus that causes COVID-19. Most people with COVID-19 get better within a few days to a few weeks after infection, so at least four weeks after infection is the start of when post-COVID conditions could first be identified. Anyone who was infected can experience post-COVID conditions. Most people with post-COVID conditions experienced symptoms days after their SARS CoV-2 infection when they knew they had COVID-19, but some people with post-COVID conditions did not notice when they first had an infection.
There is no test to diagnose post-COVID conditions, and people may have a wide variety of symptoms that could come from other health problems. This can make it difficult for healthcare providers to recognize post-COVID conditions. Your healthcare provider considers a diagnosis of post-COVID conditions based on your health history, including if you had a diagnosis of COVID-19 either by a positive test or by symptoms or exposure, as well as doing a health examination.
SYMPTOMS
People with post-COVID conditions can have a wide range of symptoms that can last more than four weeks or even months after infection. Sometimes the symptoms can even go away or come back again.
Post-COVID conditions may not affect everyone the same way. People with post-COVID conditions may experience health problems from different types and combinations of symptoms happening over different lengths of time. Most patients’ symptoms slowly improve with time. However, for some people, post-COVID conditions may last months, and potentially years, after COVID-19 illness and may sometimes result in disability.
People who experience post-COVID conditions most commonly report:
GENERAL SYMPTOMS
Tiredness or fatigue that interferes with daily life
Symptoms that get worse after physical or mental effort (also known as “post-exertional malaise”)
Fever
RESPIRATORY AND HEART SYMPTOMS
Difficulty breathing or shortness of breath
Cough
Chest pain
Fast-beating or pounding heart (also known as heart palpitations)
NEUROLOGICAL SYMPTOMS
Difficulty thinking or concentrating (sometimes referred to as “brain fog”)
Headache
Sleep problems
Dizziness when you stand up (lightheadedness)
Pins-and-needles feelings
Change in smell or taste
Depression or anxiety
DIGESTIVE SYMPTOMS
Diarrhea
Stomach pain
OTHER SYMPTOMS
Joint or muscle pain
Rash
Changes in menstrual cycles
SYMPTOMS THAT ARE HARD TO EXPLAIN AND MANAGE
People with post-COVID conditions may develop or continue to have symptoms that are hard to explain and manage. Clinical evaluations and results of routine blood tests, chest x-rays, and electrocardiograms may be normal. The symptoms are similar to those reported by people with ME/CFS (myalgic encephalomyelitis/chronic fatigue syndrome) and other poorly understood chronic illnesses that may occur after other infections. People with these unexplained symptoms may be misunderstood by their healthcare providers, which can result in a long time for them to get a diagnosis and receive appropriate care or treatment. Review these tips to help prepare for a healthcare provider appointment for post-COVID conditions.
HEALTH CONDITIONS
Some people, especially those who had severe COVID-19, experience multiorgan effects or autoimmune conditions with symptoms lasting weeks or months after COVID-19 illness. Multiorgan effects can involve many body systems, including the heart, lung, kidney, skin, and brain. As a result of these effects, people who have had COVID-19 may be more likely to develop new health conditions such as diabetes, heart conditions, or neurological conditions compared with people who have not had COVID-19.
PEOPLE EXPERIENCING ANY SEVERE ILLNESS MAY DEVELOP HEALTH PROBLEMS
PICS refers to the health effects that may begin when a person is in an intensive care unit (ICU), and which may persist after a person returns home. These effects can include muscle weakness, problems with thinking and judgment, and symptoms of post-traumatic stress disorder (PTSD). PTSDexternal icon involves long-term reactions to a very stressful event. For people who experience PICS following a COVID-19 diagnosis, it is difficult to determine whether these health problems are caused by a severe illness, the virus itself, or a combination of both.
PEOPLE MORE LIKELY TO DEVELOP LONG COVID
Researchers are working to understand which people or groups of people are more likely to have post-COVID conditions, and why. Studies have shown that some groups of people may be affected more by post-COVID conditions. These are examples and not a comprehensive list of people or groups who might be more at risk than other groups for developing post-COVID conditions:
People who have experienced more severe COVID-19 illness, especially those who were hospitalized or needed intensive care.
People who had underlying health conditions prior to COVID-19.
Some people affected by health inequities including people from racial or ethnic minority groups and people with disabilities.
HEALTH INEQUITIES MAY AFFECT POPULATIONS AT RISK FOR LONG COVID
Some people are at increased risk of getting sick from COVID-19 because of where they live or work, or because they can’t get health care. Health inequities may put some people from racial or ethnic minority groups and some people with disabilities at greater risk for developing post-COVID conditions. Scientists are researching some of those factors that may place these communities at higher risk of both getting infected or developing post-COVID conditions.
PREVENTING LONG COVID
Research suggests that people who are vaccinated but experience a breakthrough infection are less likely to report post-COVID conditions, compared to people who are unvaccinated.
However, people experiencing post-COVID conditions can seek care from a healthcare provider to come up with a personal medical management plan that can help improve their symptoms and quality of life. Review these tips to help prepare for a healthcare provider appointment for post-COVID conditions. In addition, there are many support groups being organized that can help patients and their caregivers.
Although post-COVID conditions appear to be less common in children and adolescents than in adults, long-term effects after COVID-19 do occur in children and adolescents.
CDC is working to:
Better identify the most frequent symptoms and diagnoses experienced by patients with post-COVID conditions.
Better understand how many people are affected by post-COVID conditions, and how often people who are infected with COVID-19 develop post-COVID conditions afterwards.
Better understand risk factors, including which groups might be more at risk, and if different groups experience different symptoms.
Help understand how post-COVID conditions limit or restrict people’s daily activity.
Help identify groups that have been more affected by post-COVID conditions, lack access to care and treatment for post-COVID conditions, or experience stigma.
Better understand the role vaccination plays in preventing post-COVID conditions.
Collaborate with professional medical groups to develop and offer clinical guidance and other educational materials for healthcare providers, patients, and the public.
For people who are more likely to get very sick from COVID-19 infection, medications are available that can reduce your chances of severe illness and death. Other medications can help reduce symptoms and help you manage your illness.
Here’s what you need to know.
Treating COVID-19
If you test positive and are more likely to get very sick from COVID-19, treatments are availableexternal iconexternal icon that can reduce your chances of being hospitalized or dying from the disease. Medications to treat COVID-19 must be prescribed by a healthcare provider and started as soon as possible after diagnosis to be effective. Contact a healthcare provider right away to determine if you are eligible for treatment, even if your symptoms are mild right now.
Don’t delay: Treatment must be started within days after you first develop symptoms to be effective.
People who are more likely to get very sick include older adults (ages 50 years or more, with risk increasing with older age), people who are unvaccinated, and people with certain medical conditions, such as a weakened immune system. Being vaccinated makes you much less likely to get very sick. Still, some vaccinated people, especially those ages 65 years or older or who have other risk factors for severe disease, may benefit from treatment if they get COVID-19. A healthcare provider will help decide which treatment, if any, is right for you.
The FDA has issued emergency use authorizations (EUA) for certain antiviral medications and monoclonal antibodies to treat mild to moderate COVID-19 in people who are more likely to get very sick.
Antiviral treatmentsexternal icontarget specific parts of the virus to stop it from multiplying in the body, helping to prevent severe illness and death.
Monoclonal antibodiesexternal icon help the immune system recognize and respond more effectively to the virus. They may be more or less effective against different variants of the virus that causes COVID-19.
The National Institutes of Health (NIH) provides COVID-19 Treatment Guidelinesexternal icon for healthcare providers to help them work with their patients and determine the best treatment options for them. Several options are available for treating COVID-19 at home or in an outpatient setting. They include:
Nirmatrelvir with ritonavir (Paxlovid)external icon is an investigational antiviral treatment used in adults and children ages 12 years and older. It is taken at home by mouth (orally). It should be started as soon as possible and must begin within 5 days of when your symptoms start.
Remdesivir (Veklury)external icon is an antiviral treatment used in adults and children. Treatment requires intravenous (IV) infusions at a healthcare facility for 3 consecutive days. It should be started as soon as possible and must begin within 7 days of when your symptoms start.
Bebtelovimabexternal icon is an investigational monoclonal antibody treatment used in adults and children ages 12 years and older. A healthcare provider gives bebtelovimab as a single IV injection. It should be started as soon as possible and must begin within 7 days of when your symptoms start.
Molnupiravir (Lagevrio)external icon is an investigational antiviral treatment used in adults ages 18 years and older. It is taken at home by mouth (orally). It should be started as soon as possible and must begin within 5 days of when your symptoms start.
Some treatments might have side effects or interact with other medications you are taking. To find out if medications to treat COVID-19 are right for you, you have options:
Contact your local community health center or health department
If you are hospitalized, your healthcare provider might use other types of treatments, depending on how sick you are. These could include medications to treat the virus, reduce an overactive immune response, or treat COVID-19 complications.
Managing COVID-19 Symptoms
Most people with COVID-19 have mild illness and can recover at home. If you are worried about your symptoms, the Coronavirus Self-Checker can assist in the decision to seek care. You can treat symptoms with over-the-counter medicines, such as acetaminophen (Tylenol) or ibuprofen (Motrin, Advil), to help you feel better. Learn more about what to do if you are sick.
Preventing COVID-19
COVID-19 vaccines available in the United States effectively protect people from getting seriously ill, being hospitalized, and even dying—especially people who are boosted. As with vaccines for other diseases, you are protected best when you stay up to date. CDC recommends that everyone who is eligible stay up to date on their COVID-19 vaccines, including people with weakened immune systems.
Preventive Medications
The FDA has issued an EUA for tixagevimab plus cilgavimab (Evusheld)external icon, an investigational medicine used in adults and children ages 12 years and older. Evusheld consists of 2 monoclonal antibodies provided together to help prevent infection with the virus that causes COVID-19. A healthcare provider gives Evusheld as 2 separate consecutive intramuscular (IM) injections at a doctor’s office or healthcare facility. If you are moderately or severely immunocompromised or severely allergic to COVID-19 vaccines, you may be eligible for Evusheld. Talk to a healthcare provider to determine if this option is right for you.
The right medications for COVID-19 can help. People have been seriously harmed and even died after taking products not approved for use to treat or prevent COVID-19, even products approved or prescribed for other uses. Talk to a healthcare provider about taking medications to treat COVID-19.
CDC uses Travel Health Notices (THNs) to alert travelers and other audiences to health threats around the world and advise on how to protect themselves.
On April 18, 2022, CDC updated its COVID-19 THN system. Level 4 will no longer be based on COVID-19 incidence or case count alone. It will be reserved for special circumstances, such as rapidly escalating case trajectory or extremely high case counts, emergence of a new variant of concern, and healthcare infrastructure collapse. Levels 3, 2, and 1 will still be primarily determined by 28-day incidence or case counts as outlined below.
COVID-19 Travel Recommendations can be found in two places:
The 4-level system categorizes international destinations into the following levels:
Level 4: Special Circumstances / Do Not Travel
Do not travel to this destination.
If you must travel, make sure you are up to date with your COVID-19 vaccines before your trip.
Level 3: High Level Of COVID-19
Make sure you are up to date with your COVID-19 vaccines before traveling to this destination.
If you are not up to date with your vaccines, avoid travel to this destination.
If you have a weakened immune system or are more likely to get very sick from COVID-19, even if you are up to date with your COVID-19 vaccines, talk with your clinician about your risk and consider delaying travel to this destination.
Level 2: Moderate Level Of COVID-19
Make sure you are up to date with your COVID-19 vaccines before traveling to this destination.
If you have a weakened immune system or are more likely to get very sick from COVID-19, even if you are up to date with your COVID-19 vaccines, talk to your clinician about what additional precautions may be needed before, during, and after travel to this destination.
Level 1: Low Level of COVID-19
Make sure you are up to date with your COVID-19 vaccines before traveling to this destination.
Level Unknown: Unknown Level of COVID-19
Make sure you are up to date with your COVID-19 vaccines before traveling to this destination.
If you are not up to date with your vaccines, avoid travel to this destination.
If you have a weakened immune system or are more likely to get very sick from COVID-19, even if you are up to date with your COVID-19 vaccines, talk with your clinician about your risk, and consider delaying travel to this destination.
Level 4 will be reserved for special circumstances, such as rapidly escalating case trajectory or extremely high case counts, emergence of a new variant of concern, and healthcare infrastructure collapse. Other factors that may be considered include information such as vaccination rate and hospitalization rate. CDC works with country authorities through CDC country or regional offices to gather additional data as appropriate.
Level 1-3 Travel Health Notices are determined as follows:
Primary criteria for destinations with populations over 100,000
Incidence rate (cumulative new cases over the past 28 days per 100,000 population)
New case trajectory (Have daily new cases increased, decreased, or remained stable over the past 28 days?)
Primary criteria for destinations with populations of 100,000 or less
COVID-19 case counts* (cumulative new cases over past 28 days)
New case trajectory (Have daily new cases increased, decreased, or remained stable over the past 28 days?)
*CDC does not count identified imported cases (i.e., cases in travelers who were exposed in another country) against a destination’s total.
Secondary Criteria for Determining Travel Health Notice Levels
Reported case counts and incidence rates depend on testing capacity. CDC assesses testing capacity using two secondary criteria metrics: population testing rate and test-to-case ratio. The population testing rate is the number of tests conducted per 100,000 people over 28 days. The test-to-case ratio is the number of tests conducted for each case reported during the same 28-day period. Testing data are obtained from multiple sources, including Our World in Dataexternal icon, Foundation for Innovative Diagnosticsexternal icon, and country ministries of health.
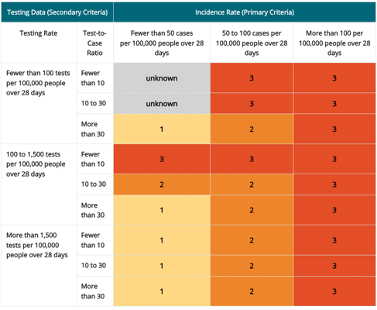
Travel Health Notice levels 1 through 3 for destinations with a population more than 100,000 people. Levels are based on combined 1) incidence rate (primary criteria) and 2) testing data (secondary criteria)
*Incidence rate is the primary criteria for destinations with a population more than 100,000 people. Testing data are the secondary criteria and that data includes both the testing rate (column 1) and test-to-case ratio (column 2). The resulting THN levels are shown in rows 3–11 of columns 3–5.
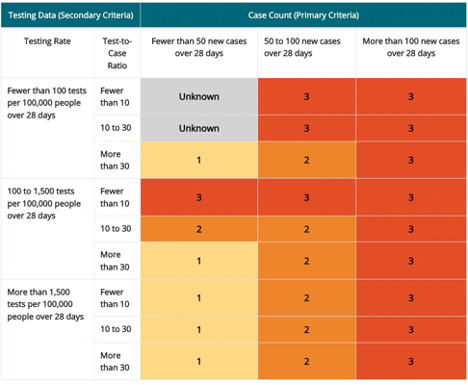
Travel Health Notice levels 1 through 3 for destinations with a population of 100,000 people or fewer. Levels are based on combined 1) case count (primary criteria) and 2) testing data (secondary criteria) *
*Case count is the primary criteria for destinations with a population fewer than or equal to 100,000 people. Testing data are the secondary criteria and that data includes both the testing rate (column 1) and test-to-case ratio (column 2). The resulting THN levels are shown in rows 3–11 of columns 3–5.
Population testing rates of more than 1,500 tests per 100,000 people over 28 days are considered sufficient to provide an accurate representation of COVID-19 in the destination. Rates less than or equal to 1,500 tests per 100,000 people over 28 days may signify concerns that testing is insufficient and may not provide an accurate representation of the incidence rate in the destination. The cutoffs for evaluating population testing ratesexternal icon have been adapted from the WHO guidelines.
The WHO determined a test-to-case ratio greater than or equal to 10 as the minimum indicator of sufficient surveillance capacity. A test-to-case ratio of less than 10 tests per case might indicate restrictive testing, or that only symptomatic people are being tested and undercounting the incidence rate (primary criteria). The preferred level is a test-to-case ratio of more than 30. The cutoffs for evaluating test-to-case ratios pdf icon[PDF – 18 pages]external icon have been adapted from the WHO guidelines.
When both the population testing rates and test-to-case ratios are high, CDC has confidence in a destination’s reported incidence. If either the population testing rate or test-to-case ratio is low, CDC has less confidence that the reported incidence accurately depicts the COVID-19 situation in the destination. In this situation, CDC adjusts a destination’s THN level as shown in the tables above. Countries with low incidence and testing rates are classified as unknown as well as countries that report data infrequently.
Level Unknown Travel Health Notices are determined as follows:
If a destination has insufficient data to make a THN level determination, its THN level is designated as “unknown”. Insufficient data means that the destination does not provide data or that the provided data are non-representative of the COVID-19 situation in the destination, making an accurate THN level determination difficult. This situation includes destinations with low COVID-19 incidence and low reported COVID-19 testing levels.
Raising a Travel Health Notice
CDC raises a destination’s THN level when the incidence rate (or case count) and testing metrics meet the THN threshold for a higher level and remain at that level for 14 consecutive days. The THN level may be raised before 14 days if there is a large increase in COVID-19 cases reported.
Lowering a Travel Health Notice
CDC lowers a destination’s THN level when the incidence rate (or case count) and testing metrics meet the THN threshold for a lower level and remain at that level for 28 consecutive days. Vaccination coverage rates and case trajectory will be considered when determining if the THN level can be lowered before 28 days.
We use cookies to ensure that we give you the best experience on our website. If you continue to use this site we will assume that you are happy with it.